Materials and Methods: This Interventional study was carried out in the Department of Paediatrics, at Centre for Woman and Child Health (CWCH) with 66 newborn (0-28 days) patients admitted as a case of suspected sepsis. Investigation and treatment were given with injectable antibiotics according to clinical diagnosis and conditions. Families who agreed to stay and complete the treatment were given the complete course of antibiotics in hospital levelled as IPD group and those who wanted to shorten their stay in hospital, were discharged with injectable antibiotics and follow up in the outpatient department as OPD group.
Results: Data was analysed on 59 neonates, 37 in the OPD and 22in the IPD group, admitted to hospital between April 2014 and December 2015. There were no readmissions or complications in either group but one newborn died in the IPD group. Cure rate was 100% in both OPD and IPD groups. Average duration of hospital stay was 3.95±1.76 days and 6.14±2.99 days in the OPD and IPD groups respectively. Treatment cost per patient was 5,823±3,752 BDT and 7,082±6,520 BDT in the OPD and IPD groups respectively. Conclusion: Early discharge with injectable antibiotics as an outpatient is a safe and cost effective option for newborn sepsis.
Key word:Antibiotic, Hospital stay, Neonate, Sepsis, Treatment cost.
Neonatal sepsis is a major cause of morbidity and mortality in developing countries with one paper stating that sepsis and pneumonia was the cause of death in 27% of newborns. The early and efficient diagnosis of neonatal sepsis remains a difficult task due to delayed development of signs and symptoms. Early diagnosis and treatment with suitable antibiotics are usually started in hospital. Although ideally antibiotic regimens should be selected on the basis of local organism isolation and antibiotic sensitivity, in reality antibiotics are chosen on the basis of broad epidemiological information about organisms in developing countries. In neonatal sepsis, treatment with combined antibiotics is given for at least 7 days, for which families have to stay in hospital for a long time with increased treatment cost. This length of stay is one of the major barriers to providing the full treatment course in neonatal sepsis in developing countries, especially for working parents.
Thus there is a need to provide treatment with injectable antibiotics in the OPD after initial treatment in hospital. It is expected that this will reduce the duration and hence the cost of hospital stay. Furthermore, families will feel more comfortable completing the full course of treatment from home. The aim of this study was to assess whether discharging newborns with sepsis to continue treatment as an outpatient with a single antibiotic (ceftriaxone , , , ) or a combination regimen that was prescribed during admission was safe and whether there was a reduction in cost.
This intervention study was carried out from April 2014 to December 2015 at CWCH in Ashulia, a peri-urban area to the northwest of Dhaka Metropolitan Area in Bangladesh. Any newborn baby (0-28 days) admitted to CWCH who had a provisional diagnosis of neonatal sepsis was included in this study. Neonates who also had hypoxic ischaemic encephalopathy (HIE), congenital heart disease, very low birth weight (<1,500 g), meconium aspiration syndrome, major congenital anomaly or birth injury (cephalhaematoma, intracranial haemorrhage) were excluded from the study. Among the 66 neonates who fulfilled the inclusion criteria, a total of 37 did not want to complete the total duration of treatment in hospital and were categorised for early discharge (OPD group) and 22 neonates were treated according to our hospital protocol in the IPD. We discussed with the parents in detail about the purpose of the study, risks, benefits, possible outcomes and took verbal consent. All the selected families participated voluntarily and their confidentiality was strictly maintained. Written ethical permission was taken from the ethical review committee of the CWCH.
After admission the neonates were assessed for features of sepsis such as convulsions, respiratory rate 60 breaths/min, severe chest indrawing, grunting, bulging fontanelle, pus draining from the ear, redness around the umbilicus, core (rectal) temperature 37.7°C or <35.5°C, lethargic or unconscious, reduced movements, not able to feed, cyanosis, digital capillary refill time>2 seconds, oxygen saturation <92%. To support the clinical suspicion of sepsis the following investigations were occasionally done-CRP (abnormal ≥6 mg/L), WBC count (abnormal<5x103/μL or >15x103/μL), total neutrophil ratio (IT ratio) (abnormal>0.2), blood CS, urine RE, C/S, CSF study and chest X-ray-and treatment started. Antibiotics were given according to standard doses used for neonatal sepsis such as Ampicillin (100 mg/kg/d), Gentamicin (7.5 mg/kg/dose), Cefotaxime (50 mg/kg/dose), Ceftriaxone (75-100 mg/kg/dose), Meropenem (40 mg/kg/dose) or Vancomycin (10 mg/kg/dose) in single or in combination regimens. After 3-4 days of initial treatment the babie's condition usually improved with good feeding or suckling and stable vital signs and they were divided into two groups-those who agreed to continue full course of treatment staying in the hospital (IPD group) and those who did not agree to stay in hospital and were discharged with injectable antibiotics and followed up as an OPD patient.
The process of discharge with injectable antibiotic and OPD follow up had the following features:
- After initial improvement (good feeding/suckling, vital signs stable) babies from the OPD group were discharged early.
- The baby was discharged with IV cannula in situ with a plan to continue antibiotics that had already been given in the IPD.
- A register book was maintained for those who came for daily injectable antibiotics.
- A medical officer (MO) examined the baby to identify any problems when they came for their injections.
- Families brought their newborns for a final follow-up seven days after completion of the antibiotic course and the final assessment was done by a paediatrician in the outpatient department.
- Parents were advised to come back to hospital immediately if they saw any deterioration in their baby.
- Communication was maintained with parents over telephone.
- Parents were counselled on how to take care of the IV cannula at home.
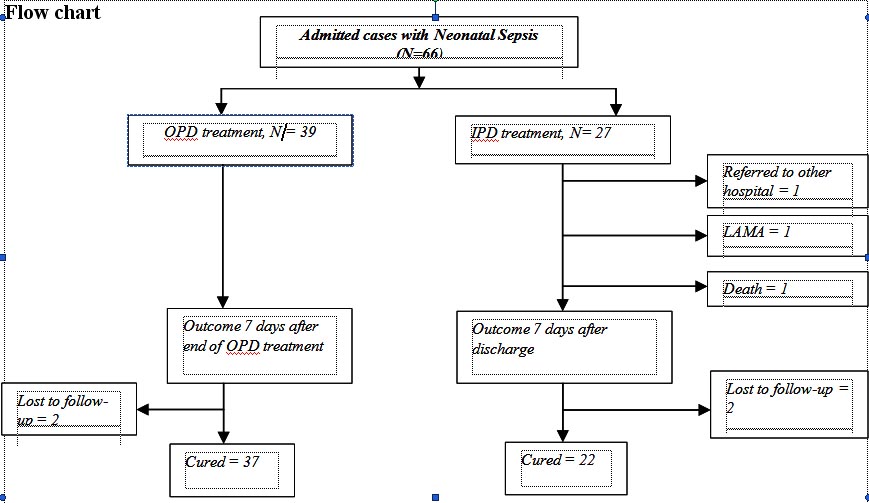
A total of 66 neonates were recruited for the study. Among them, 39 were in the OPD group and 27 in the IPD group. A total of seven patients were excluded (OPD 2 and IPD 5) due to reasons such as lost to follow-up (4), left against medical advice (LAMA) (1), death (1) and referred to a higher centre (1). Finally, data was analysed for 59 neonates (OPD 37 and IPD 22). (see Flow chart below.)
When socio demographic comparisons were made, there were no statistically significant differences between these two groups (Table I).
|
OPD |
IPD |
P value |
Household head's occupation |
|
|
|
Service |
20 (54) |
11 (52.4) |
0.44 |
Others |
11 (29.7) |
8 (38.1) |
|
Businessman |
6 (16.2) |
1 (4.8) |
|
Unemployed |
0 (0) |
1 (4.8) |
|
Neonate's Gender |
|
|
|
Male |
24 (64.9) |
12 (54.5) |
0.58 |
Female |
13 (35.1) |
10 (45.5) |
|
Mode of delivery |
|
|
|
Normal |
21 (56.8) |
13 (59.1) |
1.00 |
Caesarean |
16 (43.2) |
9 (40.9) |
|
Place of delivery |
|
|
|
CWCH |
13 (35.1) |
5 (23.8) |
0.41 |
Home |
14 (37.8) |
9 (42.9) |
|
Other facilities |
10 ((27) |
7 (33.3) |
|
There were also no statistically significant differences in the common clinical features during admission of the two groups (Table II).
|
OPD |
IPD |
P |
Admission weight |
|
|
|
<2500g |
15 (40.5) |
15 (68.2) |
0.06 |
≥2500g |
22 (59.5) |
7 (31.8) |
|
Onset of sepsis |
|
|
|
Early sepsis (within 72h) |
23 (62.2) |
13 (59.1) |
1.00 |
Late Sepsis (more than 72h) |
14 (37.8) |
9 (40.9) |
|
Not able to feed |
17 (45.9) |
14 (63.6) |
0.28 |
Oxygen saturation (≤95%) |
16 (43.2) |
10 (45.5) |
1.00 |
Convulsion |
5 (13.5) |
0 (0) |
0.15 |
Breathing difficulties (Respiratory rate≥60 breaths/min) |
8 (21.6) |
8 (36.4) |
0.24 |
|
OPD |
IPD |
P |
Severe chest indrawing |
4 (10.8) |
7 (31.8) |
0.08 |
Nasal flaring |
2 (5.4) |
7 (31.8) |
0.01 |
Reduced movement |
11 (19.7) |
11 (50.0) |
0.17 |
Grunting |
4 (10.8) |
4 (18.2) |
0.46 |
Core Temperature |
|
|
|
≥37.7°C (fever) |
5 (13.5) |
6 (27.3) |
0.21 |
<35.5°C (hypothermia) |
2 (5.4) |
1 (4.5) |
|
Normal |
30 (81.1) |
15 (68.2) |
|
Lethargic or unconscious |
7 (18.9) |
4 (18.2) |
1.00 |
No suckling at all |
3 (8.1) |
1 (4.5) |
1.00 |
Chest crepitations |
2 (5.4) |
5 (22.7) |
0.09 |
Cyanosis |
1 (2.7) |
4 (18.2) |
0.06 |
Digital capillary refill time > 3 s |
0 (0) |
2 (9.1) |
0.14 |
OBoth OPD and IPD group's cure rates were 100% and there were no readmissions or complications in either group. The average hospital stay in the OPD group was 3.95±1.76 days and in the IPD group was 6.14±2.99 days. Average (SD) hospital cost in the OPD group was 5,823±3,752 BDT and in the IPD group 7,082±6,520 BDT (Table III).
|
OPD, N=37 |
IPD, N=22 |
P value |
Average hospital stay duration (days) |
3.95±1.76 |
6.14±2.99 |
0.001 |
Average OPD antibiotic duration (days) |
3.49±1.19 |
- |
- |
Average cost (BDT) per patient |
5823±3752 |
7082±6520 |
0.35 |
There are no statistically significant differences between the two groups in the types of regimens used (Table IV).
Antibiotic |
Starting |
Final |
||
OPD, N = 37 (%) |
IPD, N = 22 (%) |
OPD, N = 37 (%) |
IPD, N = 22 (%) |
|
Ampicillin + Gentamicin |
5 (13.5) |
4 (18.2) |
3 (8.1) |
1 (4.5) |
Cefotaxime + Gentamicin |
9 (24.3) |
6 (27.3) |
6 (16.2) |
4 (18.2) |
Ceftriaxone + Gentamicin |
0 (0) |
1 (4.5) |
0 (0) |
1 (4.5) |
Cefotaxime |
5 (13.5) |
2 (9.1) |
5 (13.5) |
2 (9.1) |
Ceftriaxone |
12 (32.4) |
6 (27.3) |
18 (48.6) |
9 (40.9) |
Meropenem |
1 (2.7) |
0 (0) |
0 (0) |
2 (9.1) |
Cefotaxime + Amikacin |
1 (2.7) |
0 (0) |
2 (5.4) |
0 (0) |
Ampicillin + Flucloxacilin |
1 (2.7) |
0 (0) |
1 (2.7) |
0 (0) |
Ceftriaxone + Flucloxacilin |
2 (5.4) |
2 (9.1) |
1 (2.7) |
2 (9.1) |
Cefotaxime + Flucloxacilin |
0 (0) |
1 (4.5) |
- |
- |
Ampicillin |
1 (2.7) |
0 (0) |
- |
- |
Meropenem + Vancomycin |
- |
- |
1 (2.7) |
0 (0) |
Ciprofloxacin |
- |
- |
0 (0) |
1 (4.5) |
In both OPD and IPD patients the most commonly used antibiotic regimen was Ceftriaxone alone followed by combined Cefotaxime with Gentamicin.
Table V shows that investigations done for neonatal sepsis diagnosis were variable but this variability was not significantly different between the two groups.
Investigation |
OPD* |
IPD* |
P value |
CRP |
|
|
|
On admission (OPD=30, IPD=18) |
14 (46.7) |
8 (44.4) |
1.00 |
WBC (OPD=31,IPD=17) |
6 (80.6) |
15 (68.2) |
0.69 |
IT ratio (OPD=13,IPD=4) |
3 (23.1) |
0 (0) |
0.54 |
Blood C/S (OPD=9, IPD=5) |
4 (44.4) |
3 (60.0) |
1.00 |
CSF study (OPD=1, IPD=2) |
0 (0) |
1 (50.0) |
1.00 |
X-ray chest (OPD=3, IPD=7) |
2 (66.7) |
4 (57.1) |
1.00 |
Discussion
According to most guidelines for treatment of neonatal sepsis Ampicilin and Gentamicin are used as 1st line drugs. Ceftriaxone or Cefotaxime can be used for serious bacterial infections in the neonatal period.2 Once daily dose and its pharmacokinetics favours Ceftriaxone for use in the first three months of life. One major concern with the use of Ceftriaxone in neonates is its increased risk of hyperbilirubinemia especially in preterm babies. In our study preterm babies were excluded and we used Ceftriaxone in term mature babies without jaundice.In this study we found that there were no differences regarding cure rate, readmission or any complication between the OPD and IPD groups. In one study from a high income country, it was found that in early discharge with home injectable antibiotic therapy there were no serious complications or treatment failure; in addition, costs were lower compared with continued inpatient treatment.
The main limitation of this study was that the diagnosis of neonatal sepsis was done mainly on the basis of clinical signs and symptoms because of inadequate microbiological facilities in our hospital. All patients allocated to OPD treatment did not attend our hospital for follow up treatment. Instead, they completed the rest of their course of antibiotics in other health facilities. In these cases, we gathered information by phone.
Despite these limitations we conclude that early discharge with injectable antibiotic therapy as OPD treatment of neonatal sepsis is safe and cost-effective in developing countries.
Acknowledgments
We acknowledge all Medical Officers and nurses of the Department of Paediatrics for data collection and recording as well as the families of all newborns who participated in the study.
References
- Chowdhuri HR, Thompson S, Ali M, Alam N, Yunus M, Streatfield PK. Causes of neonatal deaths in a rural subdistrict of Bangladesh: implications for intervention. J Health Popul Nutr. 2010; 28(4):375-82.
- Darmstadt GL, Batra M, Zaidi AK. Parenteral antibiotics for the treatment of serious neonatal bacterial infections in developing country settings. Pediatr Infect Dis J. 2009; 28(1 Suppl):S37-42.
- Saez-Llorens X, McCracken GH Jr. Clinical phamacology of antimicrobial agents. In: Remington JS, Klein JO, editors. Infectious Diseases of the Fetus and Newborn Infant. 5th ed. Philadelphia, PA: WB Saunders; 2001.p.1419-1466.
- Wiese G. Treatment of neonatal sepsis with ceftriaxone/gentamicin and with azlocillin/gentamicin: a clinical comparison of efficacy and tolerability. Chemotherapy. 1988; 34:158-163.
- James J, Mulhall A, de Louvois J. Ceftriaxone - clinical experience in the treatment of neonates. J Infect.1985; 11:25-33.
- Rondanelli R, Ragazzi MB, Stronati M, Calvi M, Lombardi G, Rondini G. Pharmacokinetics of Ceftriaxone in the first three months of life. Pediatr Med Chir. 1992; 14(1):55-9.
- Wagner CL, Wagstaff P, Cox TH, Annibale DJ. Early discharge with home antibiotic therapy in the treatment of neonatal infection. J Perinatol. 2000; 20(6):346-50