1Department of Urology, Bangabandhu Sheikh Mujib Medical University (BSMMU), Dhaka, Bangladesh
![]() 10.3329/bmrcb.v45i3.44652
10.3329/bmrcb.v45i3.44652 ![]() 0000-0003-4919-9404
0000-0003-4919-9404
Background: Urolithiasis is one of the common diseases of the urinary system, with an incidence of approximately 5-10% among the general population. Among the minimally invasive surgeries, percutaneous nephrolithotomy (PCNL) is the gold standard therapy for large and/or complex renal stones.
Objective: The study was carried out to predict the stone-free rate after PCNL by using the Guy's stone score.
Methods This prospective cross-sectional study was conducted in the Department of Urology, Bangabandhu Sheikh Mujib Medical University, (BSMMU), Dhaka from February 2016 to January 2017. The patients with renal stone attending the outpatient department who met the criteria of standard PCNL.
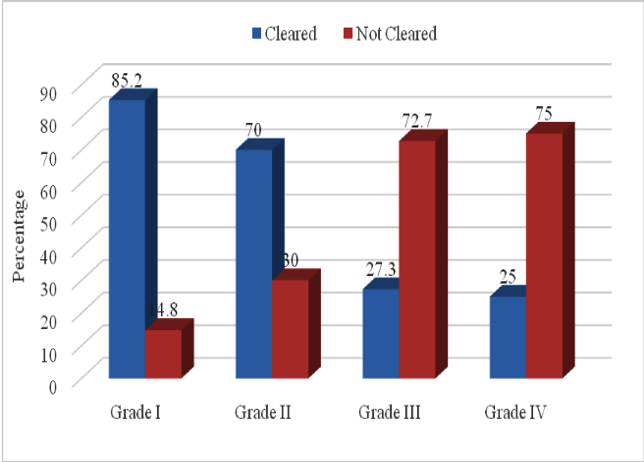
Results: A total of 52 patients with renal stone were included in this study. The mean age was to be found 45.3±14.0 with range of 18 to 73 years. Male to female ratio was 3.3:1. Almost three fourth (74.5%) patients had normal body mass index. All patients had normal anatomy. More than half 27 of the (51.9%) patients had found grade I, 10 (19.2%) Grade II, 11(21.2%) Grade III and 4 (7.7%) Grade IV. Nearly two third 34 (65.4%) patients were found total stone cleared and 18(34.6%) had residual stone. Cleared stone was found 23(85.2%) in grade I, 7(70.0%) grade II, 3(27.3%) in grade III and 1(25.0%) in grade IV.
Conclusions: Based on the study findings, it may be concluded that higher the GSS less the stone free rate.It will help in better patient counseling preoperatively, and to predict the need for ancillary treatment.
Keywords: Urolithiasis, Stone free rate, Guy's stone score, Percutaneous nephrolithotomyUrolithiasis is one of the common disease that affects the urinary system and a considerable, high-priced reason of morbidity.1 The incidence of urolithiasis is approximately 5 to 10% in the general population, and 30% of the surgical workload is related to urinary stone treatment in a urology department.2 The prevalence of urolithiasis is increased from 3.2% in the 1970s to 8.8% in 2010.3 Both in adults and children stone size and location, other factors, including stone composition, patient factors, and renal anatomy, can influence the success of specific treatment modalities.1 Over the years, minimally invasive surgeries of urinary stones become popular and currently there are many options like, percutaneous nephrolithotomy (PCNL), ureterorenoscopy, lithaloplaxy, shock wave lithotripsy (SWL), and RIRS (retrograde intrarenal surgery).
Percutaneous nephrolithotomy (PCNL) is the gold standard therapy for large and/or complex renal stones and stones in the inferior calyx.4
Greater surgeon experience and improvements in instruments (i.e., flexible pyeloscopes and ureteroscopes) as well as lithotripsy technology i.e. ultrasound/ pneumatic devices, holmium/ yttrium-aluminum-garnet laser) have increased the efficacy of PCNL, yielding stone-free rates of >90%.5
Guy's stone scoring system was easy to apply, easily reproducible and more convenient to be used in day to day practice.6 In this study, Guy's stone scoring system was applied to predict in grading stone-free rate and thus patients can be more accurately counseled preoperatively about the chance of becoming stone free after their procedure. As there is no established scoring system for prediction of (Stone free rate) SFR after PCNL in Bangladesh, this study will help in encourage in establishing GSS system for objective assessment of technical modifications (e.g. supine vs. prone) and comparing SFR of this center against the predicted SFR.
This prospective cross-sectional study was conducted in the Department of Urology, Bangabandhu Sheikh Mujib Medical University, (BSMMU), Shahbagh, Dhaka from February 2016 to January 2017. The patients with renal stone attending the outpatient department who met the criteria of standard PCNL.A total of 52 patients were included in this study through purposive sampling. The patient having previous history of open renal stone surgery, relook PCNL, post PCNL residual stone, unfit for major surgery, pregnancy, coagulation disorder, age<18years, radiolucent stone were excluded from the study. The demographic information, relevant history, clinical findings and investigation reports of all the study subjects were recorded in the data collection sheet. Any complications during the procedure and hospital admission were also recorded.
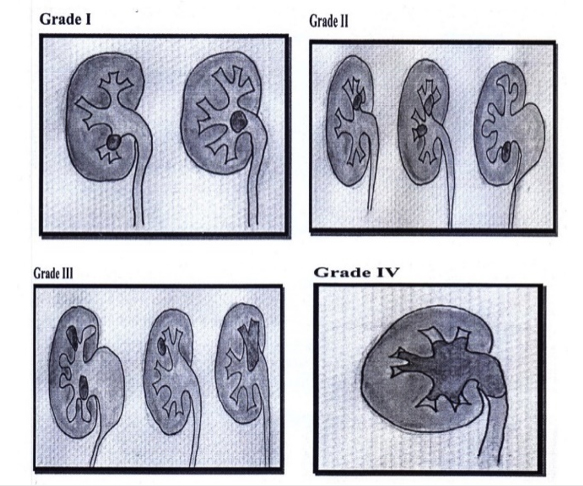
Study subjects were classified according to Guy's stone score based on the findings of preoperative IVU and per operative retrograde pyelography (RGP). The score comprised four grades:
Grade I: solitary stone in mid/lower pole or solitary stone in the pelvis with simple anatomy;
Grade II: solitary stone in the upper pole or multiple stones in a patient with simple anatomy or a solitary stone in a patient with abnormal anatomy;
Grade III: multiple stones in a patient with abnormal anatomy or stones in a caliceal diverticulum or partial stag horn calculus and
Grade IV: stag horn calculus or any stone in a patient with spina bifida or spinal injury.
The hydronephrosis due to stone was not considered as abnormal anatomy. A single person was involved in designation of Guy's Stone Score.
All PCNL procedures were done by standard technique. Initially cystoscopic insertion of ureteric catheter was done under C-arm guidance in lithotomy position using rigid cystoscope. Patients were then put in prone position and percutaneous access was obtained using C-arm fluoroscopy and retrograde contrast pyelogram. Tract dilatation was performed with Alken dilator with Amplatz sheath up to 27Fr. Nephoscopy was performed with 24 Fr rigid nephroscope (Richard Wolf, Germany) and stone fragmentation was performed with pneumatic lithoclast. At the end of the procedure, stone clearance was checked on combined fluoroscopy and nephroscopy. Antegrade double-J stent were placed in all patients. Nephrostomy tube was inserted as a routine at the end of the procedure. Nephrostomy tube was removed on first post-operative day except for second look PCNL. The patients were routinely assessed using plain abdominal radiography at 6 weeks postoperatively. The stone-free status was defined as no stones visible or the presence of clinically insignificant residual fragments <4min.
Statistical analysis: Statistical analyses were carried out using the Statistical Package for Social Sciences version 20.0 for Windows (SPSS Inc., Chicago, Illinois, USA). A descriptive analysis was performed for all data. The mean values were calculated for continuous variables. The quantitative observations were indicated by frequencies and percentages. Unpaired t-test performed to compare continuous variables between Guy's stone score and stone free rate. A p value <0.05 was considered as significant.
It was observed that mean age was found 45.3±14.0 with range 18 to 73 years and majority (34.6%) patients had belonged to age 41-50 years. Male and female ratio was 3.3:1 the body mass index distribution of the study population was 39 (75.0%) patients had belonged to 18.5-22.9 kg/m2, 8(15.4%) had 23.0-26.9 kg/m2 and 5(9.6%) had <1 8.5 kg/m2. The study population (100.0%) had normal anatomy. It was observed that 27 (51.9%) patients had found Guy's stone score grade I, among them 23(85.2%) patients had total clearance of stone, 4(14.8%) had residual stone, 10(19.2%) patients were Guy's stone score Grade II, among them7(70.0%) had total clearance of stone and 3(30.0%) had residual stone. Furthermore,11(21.2%) patients were in Guy's stone score Grade III among them 237% were stone free and 4(7.7%) patients were Grade IV only 1(25%) patient had stone clearance (table I, II and figure 1).
Guy's stone score |
Number of patients |
Percentage |
Grade I |
27 |
51.9 |
Grade 11 |
10 |
19.2 |
Grade III |
11 |
21.2 |
Grade IV |
4 |
7.7 |
Guy's score |
|
Stone free rate |
||||
|
|
Cleared |
Not cleared |
pvalue |
||
|
Total |
n |
% |
n |
% |
|
Grade I |
27 |
23 |
85.2 |
4 |
14.8 |
0.002s |
Grade II |
10 |
7 |
70.0 |
3 |
30.0 |
0.696"/ |
Grade III |
11 |
3 |
27.3 |
8 |
72.7 |
0.003s |
Grade IV |
4 |
1 |
25.0 |
3 |
75.0 |
0.083°l |
This prospective cross sectional study was carried out with an aim to predict the stone-free rate after PCNL by using the Guy's stone score. A total of 52 patients with renal stone attending the outpatient department of BSMMU hospital from February 2016 to January 2017 were selected on the basis of selection criteria were included in this study.
In this study, it was observed that 34.6% patients with renal stone had belonged to age 41-50 years. The mean age was found 45.3±14.0 with range 18 to 73 years and male female ratio was 3.3:1. Similarly, Singhania et al Muhammad et al Egilmez et a land Khawaja et al were found same age range and male predominance. In this series, it was observed that three fourth (75.0%) patients had belonged to 18.5-22.9 kg/m2, 8(15.4%) had 23.0-26.9 kg/m2 and 5(9.6%) had <18.5 kg/m2., which is consistent with the Lojanapiwat et al study, where they found more than two third of their study subjects had normal BMI.6 Similar observations regarding the normal BMI also observed in other studies.1,3,4
In this present study, it was observed that all (100.0%) patients had normal anatomy. There were no findings in abnormal anatomy. The score correlates with stone free rates but not with complications. The grading system mainly takes into consideration the number of stones, stone location and whether the renal anatomy was simple or abnormal.7 The score was based not just on the stones targeted for treatment in the particular procedure. A significant predictor was itself not a predictive tool, and some predictors, such as the pelvicalyceal system anatomy, were very difficult and time consuming to measure.2 Recently, other research groups had reported the development of prediction models for PCNL.3,11 However, the proposed models have many pitfalls, thus they were not widely used. The grades were divided by stone number, location, simple versus abnormal anatomy, and stag horn stone status.2
In this current study, it was observed that more than half (51.9%) patients had found grade I, 19.2% Grade II, 21.2% Grade III and 7.7% Grade IV.
Vicentini et al used Guy's Stone Score (GSS) to predict percutaneous nephrolithotomy outcomes in the supine position based on preoperative computed tomographic scan in 155 renal cases.12 They confirmed the usefulness of the GSS tool based on CT findings in the accuracy of evaluation of renal stones in respect of surgical outcome and complications. Thomas et alfound the distribution of cases according to the stone score was 28.0% classified as grade I, 34% as grade II, 21.0% as grade III, and 17.0% as grade IV, which is closely resembled with the present study.3
In this series, it was observed that almost two third (65.4%) patients found in total clearance of stone and 34.6% had residual stone, which is consistent with other researchers, where they found stone free rate ranges from 62.0%to 70% of their study patients.3-13,14Lojanapiwat et al found stone nephrometric scores were significantly associated with stone free status but not with postoperative complications. Noureldin et al and Okhunov et al verified that the Guy’s Stone Score was highly efficient in predicting stone-free rates even on applying computed tomography (CT). They defined SFR status as absence of residual fragment or asymptomatic fragment of s4 mm. As in the present study, they also found a significant correlation between GSS and stone-free rate.6,15-16
Conclusion
The Guy's scoring system is a simple and easily reproducible system to classify the severity of renal stones and excellent tool to predict stone-free rate. In this study, majority of patients were free from stone and among them majority belonged to grade I followed by grade II, grade III and grade IV respectively. It can be concluded that higher the GSS, less the stone free rate. Hence, it helps in better patient counseling preoperatively and helps in predicting the need for ancillary treatment.
Acknowledgement
It is of great pleasure to express my regards to my respected teacher and guide Dr. Muhammad Hossain, Associate Professor, Department of Urology, Bangabandhu Sheikh Mujib Medical University, Dhaka, for his scholastic guidance, constructive criticisms, suggestions and co-operation which made this study possible.
Conflict of Interest
None
References
- Mehmet, N.M. and Ender, O, Effect of urinary stone disease and its treatment on renal function. World Journal of Nephrology. 2015; 4:271. doi: 10.5527/wjn.v4.i2.271
- Jeong, C.W., Jung, J.W., Cha, W.H., Lee, B.K., Lee, S., et al., 2013. Seoul National University renal stone complexity scores for predicting stone-free rate after percutaneous nephrolithotomy. PLoS One. 8:65888. doi: 10.1371/journal.pone.0065888
- Thomas, K., Smith, N.C., Hegarty, N. and Glass, J.M., 2011. The Guy's stone score-grading the complexity of percutaneous nephrolithotomy procedures. Urology. 2010; 78:277-81.
- Ingimarsson, J.P., Dagrosa, L.M., Hyams, E.S. and Pais, V.M., 2014. External validation of a preoperative renal stone grading system: reproducibility and inter-rater concordance of the Guy's stone score using preoperative computed tomography and rigorous postoperative stone-free criteria. Urology. 2013; 83:45-49. doi: 10.1016/j.urology.2013.09.008
- Mandal, S., Goel, A., Kathpalia, R., Sankhwar, S., Singh, V., et al. Prospective evaluation of complications using the modified Clavien grading system, and of success rates of percutaneous nephrolithotomy using Guy's Stone Score: A single-center experience. Indian Journal of Urology, 2012; 28:392. doi: 10.4103/0970-1591.105749
- Lojanapiwat, B., Rod-Ong, P., Kitirattrakarn, P. and Chongruksut, W. Guy's Stone Score (GSS) Based on Intravenous Pyelogram (IVP) Findings Predicting Upper Pole Access Percutaneous Nephrolithotomy (PCNL) Outcomes. Advances in Urology, 2016. doi: 10.1155/2016/5157930
- Singhania, P. and Raut, N., 2016. Prediction of the Stone-Free Rates After Percutaneous Nephrolithotomy (PCNL) Using Guy's Stone Score. PARIPEX-Indian Journal of Research, 5. doi: 10.15373/22501991
- Egilmez, T. and Goren, M.R. Predicting surgical outcome of percutaneous nephrolithotomy: validation of the Guy's stone score and nephron lithometric nomogram in terms of success and complications. Journal of Clinical and Analytical Medicine. 1988; 6:281-86.
- Hossain M. Amanullah ATM. Regmi S. Rahman H. Kibria SAMG. Safety and efficacy of the supracostal access for percutaneous nephrolithotomy: Our initial experience, Bangladesh Med Res Counc Bull .2011; 37: 34-37.
- Khawaja, A.R., Dar, T.I., Sharma, A.K., Bashir, F., Tyagi, V.K. et al., 2014. Post percutaneous nephro lithotomy ynephrostogram: is it mandatory? A single I center experience. Advances in urology, 2014. doi: 10.1155/2014/423730
- Mishra S, Sabnis RB, Desai M. J Endouro, Mandal, S., Goel, A. et al., 2012. Re: Staghorn Morphometry: A New Tool for Clinical Classification and Prediction Model for Percutaneous Nephrolithotomy Mono therapy: (From: Mishra S, Sabnis RB, Desai M. J Endourol 2012; 26: 6-14. Journal of endourology, 26:1099. doi: 10.1089/end.2011.0145
- Vicentini, F.C., Marchini, G.S., Mazzucchi, E., Claro, J.F. and Srougi, M., 2014. Utility of the Guy's stone score based on computed tomographic scan findings for predicting percutaneous nephrolithotomy outcomes. Urology. 2013; 83:1248-53. doi: 10.1016/j.urology.2013.12.041
- Alobaidy, A., Al-Naimi, A., Assadiq, K., Alkhafaji, H., Al-Ansari, A. et al. Percutaneous nephrolithotomy: critical analysis of unfavorable results. The Canadian Journal of Urology. 2011; 18:5542-47.PMID: 21333049
- Pevzner, M., Stisser, B.C., Luskin, J., Yeamans, J.C., Cheng-Lucey, M. et al. Alternative management of complex renal stones. International Urology and Nephrology. 2011; 43:631-38. doi: 10.1007/s11255-010-9880-y
- Noureldin, Y.A., Elkoushy, M.A. and Andonian, S. Which is better? Guy's versus STONE nephrolithometry scoring systems in predicting stone-free status postpercutaneousnephrolithotomy. World Journal of Urology. 2015; 33:1821-25. doi: 10.1007/s00345-015-1508-5
- Okhunov, Z., Helmy, M., Perez-Lansac, A., Menhadji, A., Bucur, P., Kolla, et al. Interobserver reliability and reproducibility of STONE nephrolithometry for renal calculi. Journal of Endourology. 2013; 27:1303-06. doi: 10.1089/end.2013.0289