Mihir Kanti Adhikari
Department of Medicine, 250 bedded District Hospital, Habiganj, Bangladesh.
Shohael Mahmud Arafat
Department of Internal Medicine, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh.
Mehruba Alam Ananna
Department of Nephrology, BIRDEM General Hospital and Ibrahim Medical College, Dhaka, Bangladesh.
Md Atikur Rahman
Department of Internal Medicine, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh.
Hasan Imam
Department of Internal Medicine, Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh.
Shah Mohammad Mohaimenul Haq
Kuwait Bangladesh Friendship Government Hospital, Dhaka, Bangladesh.
Keywords: Adenosine deaminase, tuberculous lymphadenitis, FNAC, BCG
DOI: 10.3329/bmrcb.v47i2.57773
Abstract
Background: Extra-pulmonary tuberculosis often requires FNAC or biopsy of lymph node to reach a final diagnosis of tuberculous lymphadenitis, which is invasive, expensive, and needs an advanced setting. Estimation of adenosine deaminase (ADA) in different body fluid and serum has been suggested as a quick, cheap, and reliable test for tuberculosis.
Objective: The study was intended to assess the usefulness of serum ADA in the diagnosis of tuberculous lymphadenitis.
Methods: This was a cross-sectional observational study, conducted in BSMMU over a two year period and included 68 participants, divided equally into two group e.g. tuberculous lymphadenitis and a healthy comparison group. As tuberculous lymphadenitis, only newly diagnosed cases, labeled on the basis of histopathological findings of epithelioid granuloma with caseation necrosis were included. Serum ADA concentrations were estimated by enzymatic method and compared between groups.
Results: The mean serum ADA concentration was found to be 25.52±7.11 U/L in tuberculous lymphadenitis group, which was significantly higher (p=0.000) than that of the healthy comparison group (14.82±3.85 U/L). Three different cut-off values of serum ADA (18.25 U/L, 20.45 U/L, 22.15 U/L) were used to determine the best predictive value for the diagnosis of tuberculous lymphadenitis. Sensitivity and specificity of these cut off values were 91.2% and 82.4%, 79.4% and 88.2%, 67.6% and 97.1% respectively.
Conclusion: It is clearly denoted by the study that, tuberculous lymphadenitis patients has significant higher serum ADA then the healthy comparison group. This result indicates that serum ADA can be used as a useful adjunct in the diagnosis of tuberculous lymphadenitis with conventional investigations.
Keywords: Adenosine deaminase, tuberculous lymphadenitis, FNAC, BCG
Introduction
Tuberculosis (TB) is one of the oldest diseases that is affecting human over centuries. It is a virulent infectious disease worldwide and a re-emergent disease in the current developed world. TB lymphadenitis constitutes about 35 percent of extra- pulmonary tuberculosis (EPTB) and it is 15 to 20 percent of all cases of tuberculosis.1 It is almost exclusively caused by Mycobacterium tuberculosis in Bangladesh.2 Non-tuberculous mycobacterial (NTM) infection is rare here and also uncommonly reported from India.1
The diagnosis of tuberculous lymphadenitis is usually based on clinical presentation, radiological findings, and positive tuberculin or BCG tests. FNAC or biopsy of enlarged lymph node revealing granulomatous lesion with caseous necrosis helps to finalize the diagnosis, as AFB positivity has a high association with caseation necrosis in Bangladesh.3 If such specimen becomes positive for mycobacterial stain and culture, it confirms the diagnosis. Conventional AFB smears have low sensitivity and it requires a long time for M. tuberculosis to become evident in culture. Waiting for culture result to start treatment was found to be associated with higher mortality in tuberculous peritonitis.4 So, the finding of granuloma with caseation necrosis is often considered final for the diagnosis of tuberculous lymphadenitis and treatment initiated. In many other cases, the difficulties regarding obtaining biopsy specimen and histopathological study leads to empirical anti- tuberculous therapy. It is, therefore becomes imperative to find out some rapid and useful tests for the diagnosis of tuberculosis.
Adenosine deaminase (ADA) is an enzyme involved in the purine catabolism. It is also involved in proliferation and differentiation of lymphocytes, particularly T subtypes. There are several isoforms of ADA, but the prominent ones are ADA-1 and ADA-2, which are located on different gene loci.5 Physiologically, ADA-1 isoenzyme is found in all cells, with the highest concentration in lymphocytes and monocytes, whereas ADA-2 appears to be found only in monocyte.6 The sensitivity and specificity of ADA depend on the prevalence of tuberculosis in the population. In the regions with a high incidence of tuberculosis, ADA appears to be a useful marker for early diagnosis of tuberculosis. ADA-2 found to be the predominant isoforms in tuberculosis accounting for 80-90% of the activity. The isoenzyme ADA-1 is elevated in the presence of empyema and para- pneumonic effusions.7
The value of ADA as a diagnostic marker of tuberculosis has been established in numerous studies, especially in tuberculous pleural effusion, ascites, and pericardial effusion. An elevated pleural fluid ADA level predicts tuberculous pleuritis with the sensitivity of 90-100% and the specificity of 89-100%.8 Dwivedi et al. (1990) described the sensitivity of 100% and specificity of 96.6% at an ADA level >33 U/L for early diagnosis of tuberculous peritonitis, another study by Gupta et al shown 95% sensitivity and 94.1% specificity at an ADA level >30 U/L.9,10 In South Africa, a prospective study showed an ADA cut-off level of 40 U/L resulted in a test sensitivity, specificity, positive predictive value, negative predictive value, and diagnostic efficiency of 84%, 80%, 91%, 66%, and 83%, respectively in tuberculous pericarditis.11 Koh et al studied pericardial fluid ADA level along with histopathology of pericardial biopsy and found a cut- off level of 40 U/L has the sensitivity of 93% and the specificity of 97% in the diagnosis of tubercular pericardial effusion, which is similar to the study by Mathur et al. that showed 100% sensitivity and 83.3% specificity.12,13
Bangladesh is a country with a high tuberculosis burden. FNAC from lymph node and biopsy is only available in the advanced hospitals that lack in number. Furthermore, tuberculous lymphadenitis involving internal structures like mediastinal or intra-abdominal lymph nodes, CT guided or laparoscopic approach is required, which is technically demanding and difficult even in advanced centers. With such limited resources, an ideal test for tuberculosis should be economic, minimally invasive, of high accuracy and quick to perform. ADA is a simple and inexpensive colorimetric test that can be done easily with limited resource and short training. The study was intended to assess the usefulness of serum ADA in the diagnosis of tuberculous lymphadenitis.
Materials and Methods
This cross-sectional observational study was conducted in the department of internal medicine BSMMU from March 2015 to February 2017. The study included 34 patients of tuberculous lymphadenitis over 18 years and older, of both gender. Another age and gender match 34 healthy individuals were added as a comparison group. Convenient sampling technique was adopted and subjects were chosen as per inclusion and exclusion criteria. Patients presented with constitutional features of tuberculosis, like fever, weight loss, anorexia with lymphadenopathy were considered for lymph node FNAC or biopsy. Epitheloid granuloma with caseous necrosis was labeled as tuberculous lymphadenitis. Participants who had pulmonary tuberculosis or extra-pulmonary tuberculosis along with tuberculous lymphadenitis were excluded as well as metabolic derangements like hepatic, renal or electrolyte abnormality, organic or inorganic psychosis, or current pregnancy. Before starting anti-tuberculous chemotherapy, serum ADA was measured by adenosine deaminase assay kit supplied by Diazyme laboratories, CA, USA in the laboratory of the department of microbiology of BSMMU. Ethical clearance was obtained from the institutional review board of BSMMU and informed written consent was taken from all patients. Data were compiled and analyzed by SPSS. Continuous variables were analyzed using Student t-test and one way ANOVA, when and where appropriate, categorical variables were compared using the chi-square test. A p-value < 0.05 was considered statistically significant. A ROC curve was used to determine the sensitivity and specificity of serum ADA for the diagnosis of tuberculous lymphadenitis.
Results
In this study, the age range of the tuberculous lymphadenitis as well as healthy controls ranged from 18 to 60 years, the mean (±SD) age was 29.94 (±12.1) years and 30.24 (±10.2) years respectively. Among the respondents, in both of the groups’ majority were female (70.6%) (table I).
Demographic characteristics |
Tuberculous lymphadenitis (n=34) Frequency (%) |
Healthy control (n=34) Frequency (%) |
|---|---|---|
Age (years) |
||
18-20 |
10 (29.4%) |
10 (29.4%) |
21-40 |
17 (50.0%) |
17 (50.0%) |
41-60 |
7 (20.6%) |
7 (20.6%) |
Mean age (±SD) |
29.94 (±12.13) |
30.24 (±10.21) |
Gender |
||
Male |
10 (29.4%) |
10 (29.4%) |
Female |
24 (70.6%) |
24 (70.6%) |
Residence |
||
Rural |
15 (44.1%) |
19 (55.9%) |
Urban |
19 (55.9%) |
15 (44.1%) |
In tuberculous lymphadenitis group, majority of the respondents (94.1%) had fever, other predominate symptoms were loss of appetite (79.4%), weight loss (82.4%), and pain in lymph nodes (20.6%). Symptoms like cough, nausea and vomiting were present in 11.8% of patients. In this group, 8 (23.5%) of 34 participants had a history of contact with smear positive pulmonary TB patients, while 1 (2.9%) of them had a previous history of tuberculosois. In this group, most of the patients (73.5%) presented with single regional lymphadenitis and cervical lymph nodes were mostly affected (95.8%). The largest lymph nodes were >2cm in 50% of patients. Consistency was firm in the majority (85.3%) of patients, 44.1% of them had matted lymphadenitis. Cold abscess with discharging sinus was found in 14.7% of cases. In tuberculous lymphadenitis group, mean serum ADA concentration was found to be 25.52 (±7.11) U/L and in the healthy comparison group it was 14.82 (±3.85) U/L (table a!). In the male participants, mean serum ADA was 26.23 (±10.12) U/L and in the female, it was 25.22 (±5.66) U/L (table II).
GROUP |
Mean (±SD) |
Min |
Max |
P value |
t |
|---|---|---|---|---|---|
Tuberculous lymphadenitis |
25.52 (±7.11) |
14.10 |
41.30 |
0.000a |
7.714 |
Healthy group |
14.82 (±3.85) |
8.30 |
23.90 |
|
|
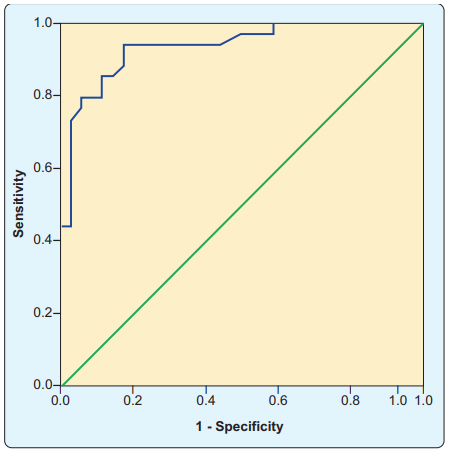
The receivers operating characteristic (ROC) curve was utilized. The area under the curve (AUC) was significant (935). The sensitivity and specificity of serum ADA in the diagnosis of tuberculous lymphadenitis for different cut off values were estimated (table III and Figure 1).
Cut of value of serum ADA |
Sensitivity |
Specificity |
|---|---|---|
18.25 (U/L) |
91.2 |
82.4 |
20.45 (U/L) |
79.4 |
88.2 |
22.15 (U/L) |
67.6 |
97.1 |
Discussion
Tuberculous lymphadenitis is the most prevalent form of extra-pulmonary tuberculosis. The final diagnosis needs FNAC or biopsy, and is difficult due to the invasiveness of the procedure and its unavailability is the low resource setting. Estimation of ADA in different body fluids is a simple method of investigation and is proved to be diagnostic. Previous studies have also shown the usefulness of serum ADA in pulmonary tuberculosis and in limited cases of EPTB.
Among the respondent, in tuberculous lymphadenitis group, most were females (70.6%), such female predilection has also been reported by previous studies.14,15 Most (79.4%) of respondents of this group was within 18 to 40 years of age. Many previous studies also reported its predominance in children and young adults.14,15 Majority of the respondents (94.10%) of this group had fever, but objective evidence of raised body temperature was found in 55.90% of cases. It can be explained by the natural history of disease; tuberculosis causes evening rise of temperature but as most of the cases was taken from outdoor at morning, elevated temperature couldn’t be demonstrated. In tuberculous lymphadenitis group, most of the patients (73.5%), presented with single regional lymph node enlargement, among them cervical lymph node involvement was most common (95.8%), which is consistent with previous studies.15,16
In this study, mean serum ADA concentration was found to be significantly higher in tuberculous lymphadenitis group (25.52 ±7.11 U/L) than the healthy comparison group (14.82 ±3.85 U/L) (p=0.000). This finding is consistent with a previous study who found mean serum ADA concentration as 20.2 (±3.64) U/L and 14.95 (±3.22) U/L in tuberculous lymphadenitis and healthy control respectively.17 Giusti have also shown serum ADA in healthy population as 17.05 (±3.75) U/L.18 Another study in Belgrade, Serbia, Stevanovic et al. found serum ADA concentration 31 (±11) U/L in a group of patients of extrapulmonary tuberculosis, of whom 27% was tuberculous lymphadenitis.19 A recent study described elevation of serum ADA level to a range of 31-40 U/L in 65% of cases and 41-60 U/L in 20% of cases in a group consisting of 30 cases of tuberculous lymphadenitis.20 These concentrations were much higher than the findings of the current study.
Three different cut-off values of serum ADA (18.25 U/ L, 20.45 U/L, 22.15 U/L) were used to determine the best predictive value for the diagnosis of tuberculous lymphadenitis in the current study. Sensitivity and specificity of these cut off values were 91.2% and 82.4%, 79.4% and 88.2%, 67.6% and 97.1% respectively. Receivers operating characteristic (ROC) curve shown area under the curve (AUC) was significant (.935) (figure 1).
We admit few limitations of our study like small sample size and convenient sampling technique. For the diagnosis of tuberculous lymphadenitis, the case definition of the presence of granuloma with caseation necrosis in FNAC or biopsy was used. Serum total ADA was measured in this study, which is less specific than ADA 2 for the diagnosis of tuberculous lymphadenitis.
Conclusion
This study clearly demonstrated significant elevation of serum ADA concentration in the tuberculous lymphadenitis patients in comparison to the healthy control. This result indicates that serum ADA can be a useful adjunct in the diagnosis of tuberculous lymphadenitis with conventional investigations. To overcome the limitations of this study a large scale multicenter study with random sampling and using culture positivity of Mycobacterium tuberculosis from FNA or biopsy material of lymph nodes as gold standard can be done. Serum ADA 2 concentration, which is more specific to tuberculosis, can also be measured.
Acknowledgments
Prof. ABM Abdullah and Prof. MA Jalil Chowdhury.
References
- Sharma SK, Mohan A. Extrapulmonary tuberculosis. Indian J Med Res. 2004;316-53.
- Nakajima C, Rahim Z, Fukushima Y, Sugawara I, Zanden AGM Van Der, Tamaru A. Identification of Mycobacterium tuberculosis clinical isolates in Bangladesh by a species distinguishable multiplex PCR. BMC Infectious Diseases. 2010;10:118.
DOI:10.1186/1471-2334-10-118 - Parveen K, Momen A, Kobra K. Frequency of Tuberculosis in Patients with Enlarged Lymph Nodes and its cost- effective first line of Diagnosis in our Country. J Dhaka National Med Coll Hos. 2011;17:34-39
- Chow KM, Hung LCT, Wong SM, Szeto CC, Chow VCY. Tuberculous Peritonitis–Associated Mortality Is High among Patients Waiting for the Results of Mycobacterial Cultures of Ascitic Fluid Samples. Clin Infect Dis [Internet]. 2002;35:409-13.
DOI:10.1086/341898 - Hirschhorn R, Ratech H. Isozymes of adenosine deaminase. Isozymes Curr Top Biol Med Res. 1980;4:131-57.
- Ungerer JPJ, Vermaak WJH. Serum Adenosine Deaminase: Isoenzymes and Diagnostic Application. Clin Chem. 1992; 38:1322-26.
- Carstens ME, Burgess LJ, Maritz FJ, Taljaard JJF. Isoenzymes of adenosine deaminase in pleural effusions/: a diagnostic tool/ ? Int J Tuberc Lung Dis. 1998;2:831-35.
- Alrokayan S. Adenosine deaminase an aid to diagnose tuberculosis. J Med Sci. 2003;3:30-45.
DOI:jms.2003.30.45 - Dwivedi M, Misra SP, Misra V, Kumar R. Value of adenosine deaminase estimation in the diagnosis of tuberculous ascites. Am J Gastroenterol. 1990;85:1123-25
- Gupta VK, Mukherjee S, Dutta SK, Mukherjee P. Diagnostic evaluation of ascitic adenosine deaminase activity in tubercular peritonitis. J Assoc Physicians India. 1992;40:387–89.
- Reuter H, Burgess LJ, Carstens ME, Doubell AF. Adenosine deaminase activity-more than a diagnostic tool in tuberculous pericarditis: cardiovascular topic. Cardiovasc J South Africa. 2005;16:143–47.
- Koh KK, Kim EJ, Cho CH, Choi MJ, Cho SK, Kim SS, et al. Adenosine deaminase and carcinoembryonic antigen in pericardial effusion diagnosis, especially in suspected tuberculous pericarditis. Circulation. 1994;89:2728-35.
DOI:10.1161/01.CIR.89.6.2728 - Mathur PC, Tiwari KK, Trikha S, Tiwari D. Diagnostic value of adenosine deaminase (ADA) activity in tubercular serositis. Indian J Tuberc. 2006;53:92-95.
- Dandapat MC, Mishra BM, Dash SP, Kar PK. Peripheral lymph node tuberculosis: a review of 80 cases. Br J Surg. 1990;77:911-12.
DOI:10.1002/bjs.1800770823 - Thompson MM, Underwood MJ, Sayers RD, Dookeran KA, Bell PRF. Peripheral tuberculous lymphadenopathy: a review of 67 cases. Br J Surg. 1992;79:763-64.
DOI:10.1002/bjs.1800790815 - Kanlikama M, Mumbuç S, Bayazit Y. Management strategy of mycobacterial cervical lymphadenitis. J Laryngol Otol. 2000;114:274–78.
DOI:10.1258/0022215001905544 - Al-nahari AM. Serum adenosine deaminase activity in patients with pulmonary tuberculosis, tuberculous lymphadenitis and tuberculois pleural effusion. Assiut Univ J Zool. 2009;38:1-9.
- Giusti G, Galanti B. Colorimetric method. Methods Enzym Anal Weinheim Verlag Chemie. 1984;315-23.
- Stevanovic G, Pelemis M, Pavlovic M, Lavadinovic L, Dakic Z, Milosevic I. Significance of adenosine deaminase serum concentrations in the diagnosis of extra-pulmonary tuberculosis. J IMAB. 2011;17:130-34.
- Sulakshana MS, Ahmed SM, Jayakumar CK. Study of serum adenosine deaminase levels in FNAC confirmed cases of tuberculous lymphadenitis. Int J Recent Adv Multidiscip Rsearch. 2015;02:0476-80.
250 bedded District Hospital, Habiganj, Bangladesh.
giash16@gmail.com
 0000-0001-7872-8761
0000-0001-7872-8761
Submission
05 March 2020
Accepted
30 June 2021
Published
01 August 2021
Apply citation style format of Bangladesh Medical Research Council
Issue
Vol 47 No 2 (2021)
Section
Research Articles
Ethical Clearance
IRB of Bangabandhu Sheikh Mujib Medical University (BMSSU), Dhaka, Bangladesh.
Financial Support
Partly by the thesis grant from Bangabandhu Sheikh Mujib Medical University (BMSSU), Dhaka, Bangladesh.
Conflict of Interest
None declared.