Syed Shahidul Islam
Department of Orthopaedic Surgery, National Institute of Traumatology and Orthopedic Rehabilitation, Dhaka, Bangladesh.
Md. Samiul Islam
Department of Orthopaedic Surgery, National Institute of Traumatology and Orthopedic Rehabilitation, Dhaka, Bangladesh.
Sultana Parvin
Department of Medicine, Sheikh Russel National Gastroliver Institute and Hospital, Dhaka, Bangladesh.
Susmita Islam
Department of Physical Medicine, National Institute of Traumatology and Orthopedic Rehabilitation, Dhaka, Bangladesh.
Rayhan Hamid
Department of Physical Medicine, National Institute of Traumatology and Orthopedic Rehabilitation, Dhaka, Bangladesh.
Md. Abdul Gani Mollah
National Institute of Traumatology and Orthopedic Rehabilitation, Dhaka, Bangladesh.
Keywords: Open fracture tibia, Injury characteristics, Infection, Antibiotic resistance.
DOI: 10.3329/bmrcb.v47i2.57781
Abstract
Background: Open fractures are a frequent occurrence in the in accident and emergency department that requires immediate care. As a pedal bone, the tibia is very prone to accidental injury, easily becomes bare following the trauma and very prone to infection. Updated knowledge about microbial aspects of open tibia fracture infection is essential for proper management.
Objective: This study evaluated the injury characteristics and resistance patterns of microorganisms involved in the infection of open fracture tibia in a single-centred study.
Methods: This was a cross-sectional study on a total of 384 patients presented at the emergency department with open fractures of the tibia (all Gustilo types) from January 2020 to July 2020 at the National Institute of Traumatology and Orthopedic Rehabilitation (NITOR), Bangladesh. Three successive culture sensitivity tests were carried out-one at the emergency room (surveillance culture), 2nd at the emergency theatre after debridement and third at ward after 1 week (7 to 10 days).
Results: Average age of the patients was 36.2± 15.5 years, with motor vehicle accidents being the predominant cause (72.9%). Gustilo III fractures were most prevalent (54.4%). The maximum infection rate was in Gustilo IIIB Fractures (40.4%). There was a significant difference in contamination rate between on admission culture (37.0%) and post debridement culture (26.3%). The infection rate from the ward samples was 44.5 %, where the postdebidement contamination was less only 26.3%. But from the ward sample, it again increased to 44.5%. Among the patient entering the ward after debridement with no contamination (73.7%) became infected in 34.62% cases, which indicates hospital-acquired infection. The bacterial resistance patterns from the ward samples were more virulent with multidrug resistance, predominantly Pseudomonas spp. and Kliebsiella spp.
Conclusion: The present study provided insight into the injury characteristics and infection patterns of open fractures of the tibia. Early debridement reduced the contamination, but there was still hospital-acquired infection with more virulent multidrug resistance phenotypes.
Keywords: Open fracture tibia, Injury characteristics, Infection, Antibiotic resistance.
Introduction
Open fractures frequently result from high - energy trauma and very often complicated by potentially fatal injuries.1, 2 Open fractures are characterized by soft tissue injury that occurs in communication of the fracture site with the outside environment. This leads to not only contamination of the fracture site with external microorganisms also the introduction of foreign bodies into the wound.1
The injury mechanism significantly influences the microbiological profile on the wound site (road traffic accident, agricultural injury, fall from height, gun-shot injury). It is well regarded that many infections in open fractures are very often nosocomial. This is because, on many occasions, causative microorganisms found inward samples cultures are different from initial surveillance culture at admission.3-5 The risk of infection can, therefore, also be influenced positively by the operating technique (e.g., debridement, instrumentation, fracture fixation, irrigation) as well as the indoor atmosphere at ward.6-8 These infections lead to malunion, nonunion, chronic osteomyelitis and sometimes even ultimate amputation.1,9
Tibial shaft fractures account for 2% of all fractures and 44,4% of all open long-bone fractures in adults.10, 11 Due to the specific anatomical features of the tibia (limited soft coverage) more than 15% of its’ fractures are classified as open and have made most infection- prone bone of the body.10 The Gustilo classification system is used widely to grade open fractures. The infection rate of open fractures varies with the fracture characteristic. Infection rates progressively increased from 0% to 2% for Gustilo type-I, 2% to 10% for type- II, and 10% to 50% for type-III.9 Management of open fractures is based on the principles that include assessment of the patient, classification of the injury, antibiotic therapy, debridement and wound management, fracture stabilization, early bone grafting, and supplemental procedures to achieve healing.8,9,12 Surgical debridement is considered the most critical step for open lower limb fracture management.
This infection complication and antibiotic resistance synergistically pose a significant threat to the health care system. It not only increases the risk for complications, but extended hospital stay and economic burden to the hospital resources put an unexpected load to the citizen as well as the Government.6 Updated knowledge about all these aspects of open tibia fracture is essential for proper management. The present study has evaluated injury characteristics and resistance patterns of microorganisms involved in the infection of open fracture tibia in a single-centre cross-sectional study among the Bangladeshi population.
Materials and Methods
This was a cross-sectional study conducted between January 2020 to July 2020 at the National Institute of Traumatology and Orthopaedic Rehabilitation (NITOR), Sher-E-Bangla Nagar, Dhaka where patients of all ages and both the sexes presented with open fractures of tibia attending emergency, were studied. Sample size of this study was 384. Purposive sampling (non randomised) according to availability of the patients and strictly considering the inclusion and exclusion criteria were done. From Admission till discharge three successive culture sensitivity test were done. Cultures were initial culture/surveillance culture (culture sample from initial wound before prophylactic antibiotic), post debridement culture (last saline irrigation in emergency theater) and finally infection culture (7 to 10 days after admission).
Approval from the Institutional Review Board (IRB) of National Institute of Traumatology and Orthopaedic Rehabilitation (NITOR), Sher-E-Bangla Nagar, Dhaka was taken to conduct this study. Keeping compliance with Helsinki Declaration for medical research involving human subject 1964, the study subjects were informed verbally about the study design, the purpose of the study and right for withdrawing themselves from the project at any time, for any reason. Individual who gave informed written consent to participate voluntarily in the study were included as a study sample.
Data were collected in a structured data collection form filled up by the investigator containing all the variables of interest according to inclusion criteria after taking their permission regarding participation and this research work. At arrival of the patients, time of hospital admission, demographic variables, date and time of injury were noted along with mechanism of injury, Gustilo types and subtypes and fracture injury characteristics. During initial resuscitation at emergency room, surveillance culture sample (from wound before prophylactic antibiotic) was collected and sent to lab. Prophylactic antibiotics (intravenous Flucloxacillin and 3rd generation cephalosporin) was administered. Then patients were sent to emergency theatre for wound debridement, fracture stabilization and soft tissue care. Debridement was done following current practice at NITOR using chlorhexidine (Hexi scrub), normal saline, hydrogen peroxide and povidone-iodine solution. A second post debridement culture (last saline wash from the wound at emergency theatre) was sent. From the theatre after initial fracture stabilisation. Stable patients were sent to post- operative ward followed by to general ward. A third infection culture sample after admission in the ward at 7 to 10 days was sent for culture sensitivity and identification of organism. Results of all culture were noted in same structured data collection form.
The data were tabulated and quantitative parameters such as age of patient were summarized in terms of mean with standard deviation and percentage, X2-statistic was applied to see significant difference between variables. The significance of the results was determined in 95% confidence interval and a value of p<0.05 considered to be statistically significant.
Results
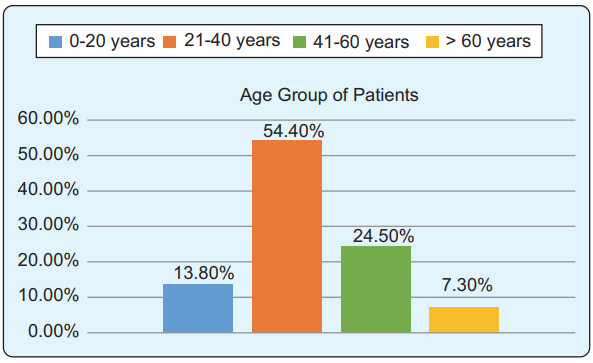
In present study among 384 studied patients, most (209) were from 21-40 years age group, in contrast with the least number of patients (28) from the elderly (>60 years) group (Figure 1). Of them, 345 were male and 39 were female. Regarding Injury Characteristics, according to Gustilo classification, Gustilo type III fracture were predominant, 99(55.3%) followed by type II, 56(31.3%) and among Gustilo subtypes Gustilo III Subtypes, specifically IIIA were predominant, 48(26.7%) followed by IIIB, 43(24.0%). (table-I).
Type of Fracture |
Frequency (Main types) |
|
Frequency (subtypes) |
|---|---|---|---|
Gustilo I |
55(14.3) |
|
|
Gustilo II |
120(31.3) |
|
|
Gustilo III |
209(54.4) |
Gustilo IIIA |
105(27.3) |
|
|
Gustilo IIIB |
91(23.7) |
|
|
Gustilo IIIC |
13(3.4) |
Total |
384(100) |
|
209(54.4) |
142 patients (37.0%) had contamination in surveillance culture while the rest 242 had no organism. Noticeably, rate of infection was largely influenced by wound debridement. In post debridement culture, only 101 (26.3%) patients had contamination compared to around 283(73.7%) with no organism in post debridement wound. But from the ward sample it again increased to 171(44.5%) cases of organism positive (table-II).
Organism Present or absent |
Surveillance culture (on arrival) Freq % |
Post debridement Culture (at emergency Theater) |
Third (infection) Culture from the wards) Freq % |
|||
|---|---|---|---|---|---|---|
Present |
142 |
37.0 |
101 |
26.3 |
171 |
44.5 |
Absent |
242 |
63.0 |
283 |
73.7 |
119 |
31.0 |
Total |
384 |
100% |
384 |
100 |
*290 |
75.5 |
The highest infection rate was in Gustilo type III, 130(76.0%) followed by type II, 39 (22.8%). While in subtypes, type IIIB is the predominant, 69 (40.4%), followed by type IIIA, 58(33.9%). (table-III).
Type of Fracture |
Frequency (Main types) |
|
Frequency (subtypes) |
|---|---|---|---|
Gustilo I |
2(1.2) |
|
|
Gustilo II |
39(22.8) |
|
|
Gustilo III |
130(76.0) |
Gustilo IIIA |
58(33.9) |
|
|
Gustilo IIIB |
69(40.4) |
|
|
Gustilo IIIC |
3(1.8) |
Infection Absent |
119(31.0) |
|
|
Wound healed Cases |
94 (24.5%) |
|
|
Total |
384(100) |
|
|
A total of 15 different type of organisms (bacteria) found in three successive cultures. Number of organisms decreased in 2nd culture (194 decreased to 138) after debridement but again increased in 3rd culture (219 in the samples from the ward). (table-IV).
Sensitivity |
|
Stap. |
Strept. |
Ecoli |
Pseud. |
Klebs. Citrob. |
Prote. |
Acine |
Serra. |
Prov. |
Entero. |
Flav. |
Plesio. |
Aero. |
Morga. |
Total |
|
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
1st Culture |
Freq |
19 |
7 |
34 |
38 |
34 |
5 |
7 |
32 |
1 |
2 |
14 |
1 |
0 |
0 |
0 |
194 |
|
% |
9.8 |
3.6 |
17.5 |
19.6 |
17.5 |
2.6 |
3.6 |
16.5 |
0.5 |
1.0 |
7.2 |
0.5 |
0 |
0 |
0 |
100 |
2nd Culture |
Freq |
6 |
6 |
23 |
35 |
26 |
3 |
8 |
18 |
1 |
1 |
9 |
0 |
1 |
1 |
0 |
138 |
|
% |
4.3 |
4.3 |
16.7 |
25.4 |
18.8 |
2.2 |
5.8 |
13 |
0.7 |
0.7 |
6.5 |
0 |
0.7 |
0.7 |
0 |
100 |
3rd Culture |
Freq |
5 |
4 |
17 |
109 |
52 |
0 |
12 |
12 |
0 |
3 |
4 |
0 |
0 |
0 |
1 |
219 |
|
% |
2.3 |
1.8 |
7.8 |
49.8 |
23.7 |
0 |
5.5 |
5.5 |
0 |
3 |
4 |
0 |
0 |
0 |
1 |
100 |
Stap. - Staphylococcus aureus |
Serra. - Serratia sp. |
||||||||||||||||
Strept. - Streptococcus sp. |
Prov. - Providencia alcalifaciens |
||||||||||||||||
Ecoli. - Escherichia coli |
Entero. - Enterobacter sp. |
||||||||||||||||
Pseud. - Pseudomonas sp. |
Flav. - Flavobacterium |
||||||||||||||||
Klebs. - Klebsiella sp. |
Plesio. - Plesiomonas sp. |
||||||||||||||||
Citrob. - Citrobacter freundii |
Aero. - Aeromonas |
||||||||||||||||
Prote. - Proteus sp. |
Morga. - Morganella moganii |
||||||||||||||||
Acine. - Acinetobacter |
|
||||||||||||||||
Gram-negative organisms were predominant with multidrug resistance. Pseudomonas and Klebsiella species are only sensitive to intravenous imipenem or meropenem only around 50-60% which is the highest sensitivity of all used drugs for these two organisms in this study. Less commonly used antibiotic Co-trimoxazole and Chloramphenicol showed good sensitivity against Staphylococcus Aureus 90-93% and E. coli 65-70%. But they are not effective against Pseudomonas and Klebsiella species (table-V).
|
Antimicrobial agent’s sensitive (S) / Intermediate (I) / Resistance (R) |
|||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
Staphylococcus aureus % |
Escherichiacoli % |
Pseudomonas spp. % |
Klebsiella spp. % |
|||||||||
S |
I |
R |
S |
I |
R |
S |
I |
R |
S |
I |
R |
|
Ampicillin |
35.3 |
00 |
64.7 |
3.1 |
00 |
96.9 |
1.7 |
00 |
98.3 |
00 |
00 |
100 |
Amoxicillin |
35.3 |
00 |
64.7 |
3.1 |
00 |
96.9 |
1.7 |
00 |
98.3 |
2.4 |
00 |
97.6 |
Piperacillin |
64.7 |
5.9 |
29.4 |
31.3 |
9.4 |
59.4 |
20.5 |
36.8 |
42.7 |
13.3 |
6.0 |
80.7 |
Cephalexin |
64.7 |
00 |
35.3 |
15.6 |
00 |
84.4 |
11.1 |
00 |
88.9 |
15.7 |
00 |
84.3 |
Ceftriaxone |
47.1 |
00 |
52.9 |
37.5 |
3.1 |
59.4 |
5.1 |
2.6 |
92.3 |
16.9 |
00 |
83.1 |
Ceftazidime |
52.9 |
11.8 |
35.3 |
40.6 |
3.1 |
56.3 |
22.2 |
1.7 |
76.1 |
22.9 |
4.8 |
72.3 |
Cefepime |
17.6 |
23.5 |
58.8 |
40.6 |
9.4 |
50.0 |
32.5 |
00 |
67.5 |
15.7 |
6.0 |
78.3 |
Cefixime |
17.6 |
11.8 |
70.6 |
28.1 |
00 |
71.9 |
5.1 |
0.9 |
94.0 |
14.5 |
00 |
85.5 |
Imipenem |
88.2 |
00 |
11.8 |
78.1 |
9.4 |
12.5 |
53.8 |
0.9 |
45.3 |
62.7 |
25.3 |
12.0 |
Meropenem |
89 |
00 |
11 |
87.5 |
9.4 |
3.1 |
47.9 |
8.5 |
43.6 |
66.3 |
12.0 |
21.7 |
Gentamicin |
88.8 |
00 |
11.2 |
75 |
00 |
25 |
23.9 |
0.9 |
75.2 |
34.9 |
00 |
65.1 |
Amikacin |
94.1 |
00 |
5.9 |
71.9 |
3.1 |
25 |
42.7 |
4.3 |
53.0 |
51.8 |
1.2 |
47.0 |
Netilmicin |
100 |
00 |
00 |
78.1 |
00 |
21.9 |
35.0 |
9.4 |
55.6 |
38.6 |
8.4 |
53.0 |
Doxycycline |
88.2 |
5.9 |
5.9 |
53.1 |
3.1 |
43.8 |
17.1 |
9.4 |
73.5 |
33.7 |
6.0 |
60.2 |
Ciprofloxacin |
58.8 |
5.9 |
35.3 |
50 |
15.6 |
34.4 |
38.5 |
3.4 |
58.1 |
26.5 |
21.7 |
51.8 |
Levofloxacin |
64.7 |
5.9 |
29.4 |
59.4 |
3.1 |
37.5 |
33.3 |
6.0 |
60.7 |
54.2 |
7.2 |
38.6 |
Moxifloxacin |
58.8 |
11.8 |
29.4 |
46.9 |
12.5 |
40.6 |
27.4 |
1.7 |
70.9 |
30.1 |
15.7 |
54.2 |
Cotrimoxazole |
88.2 |
00 |
11.8 |
65.6 |
3.1 |
31.3 |
18.8 |
00 |
81.2 |
27.7 |
1.2 |
71.1 |
Chloramphenicol |
94.1 |
00 |
5.9 |
68.8 |
00 |
31.3 |
12.8 |
6.8 |
80.3 |
55.4 |
2.4 |
42.2 |
Azithromycin |
52.9 |
00 |
47.1 |
21.9 |
9.4 |
68.8 |
13.7 |
6.8 |
79.5 |
3.6 |
4.8 |
91.6 |
Discussion
Open fracture tibia is one of the commonest emergency admissions in orthopaedic surgery.13 Exposure and contamination of the open fracture with environmental microorganisms are widespread.14 Tibia as a pedal bone, being mostly subcutaneous it is very prone to accidental injury and easily become bare following the trauma. An updated knowledge about injury characteristics and the resistance pattern of microorganisms involved in infection is the much required area of open fracture tibia management.
In this study, it was observed that the mean age of the patient was 36.2±15.5 years. An epidemiological study for 7 years on tibia fracture and another related study on Bangladeshi population also found similar mean age.15,16 In another study conducted in Brazil, the mean age of the patients with open fractures was 36±12.60 years.17 The results of all these studies are similar to our study. There were 345(89.8%) male and 39(10.2%) female patients in our study, which states of male predominance. Several related studies has reported male predominance.18,15,19
Considering injury characteristics according to Gustilo and Anderson classification found Gustilo type III fracture were predominant (54.4%) followed by type II (31.3%) and among the Subtypes IIIA were predominant (27.3%) followed by IIIB (23.7%.). A quantitative descriptive study conducted at ULBRA university hospital in Canoas, Rio Grande do Sul, Brazil, found similar type injury characteristics, which is in agreement with this study.17 A review article comprising 32 articles of 3036 patients of tibia also found same type Gustilo III predominance. Still, among the subtypes, IIIB was the highest subtype, while in our study, it is IIIA.10 But this difference is minimum.
In this study infection rate of the Gustilo type III fracture was the highest (76.0%) followed by Type II 22.8% and among the subtypes, IIIB having the most top (40.4%) then IIIA (33.9%). A study conducted at Hospital de Pronto Socorro de Canoas found a similar type of finding with the highest infection rate in Gustilo type III fracture.17 A retrospective clinical analysis of 50 patients who underwent tibial open fracture treatment found infection rate highest in Gustilo type III fractures. This finding is similar to our study, but they differ in the infection rate of subtypes, where they found Gustilo type IIIA having the highest rate.20 Their sample size is around 1/7 of ours (50 versus 384). It may be an important factor of influence.
This study found only 26.3 % contamination in the wound after debridement. According to EFFORT open reviews, surgical debridement is considered as the pivotal and most essential procedures to reduce bacterial load in open lower limb fractures.21 The infection rate from the ward samples was 44.5 %, where the post-debridement contamination was less (26.3%). Among the patient entering the ward after debridement with no contamination (73.7%) became infected in 34.6% cases, which indicates hospital- acquired infection. An observational study conducted in a tertiary hospital in India over a one-and-a-half- year period has shown that nosocomial infections are a significant issue worldwide, ranging from 1% in a few European and American countries to more than 40% in Asia.22
The bacteriological study found common organisms present in our study in three cultures were Escherichia coli, Pseudomonas spp. and Klebsiella spp. A related microbiological study of wound from All India Institute of Medical Sciences, India also reported Gram- negative organisms were predominant, which is almost similar with this study.23 A prospective multicentered study on open fracture tibia at the various hospitals of Bangladesh done by Ali et al. (2017) found Staphylococcus aureus and Streptococcus pyogenes as dominant infecting organisms. This finding differs from our study findings. It may be due to they had a very small sample size of 12 cases.16
In the present study, common gram-negative and gram-positive organisms alarmingly multidrug- resistant. Pseudomonas and Klebsiella species are only sensitive to intravenous imipenem or meropenem only around 50-60%, which is the highest sensitivity of all used drugs for these two organisms in this study.
Amikacin is the next sensitive drug having only 40- 50% sensitivity. Older dug Chloramphenicol was more than 55% sensitive for Klebsiella species. In the case of E. coli sensitivity of these four drugs was around 70-88% and for gram-positive bacteria Staphylococcus aureus 90-95%, but in the case of Netilmicin, the sensitivity is 100% for Staphylococcus aureus. Nowadays less commonly used antibiotic Co-trimoxazole and Chloramphenicol showed good sensitivity against Staphylococcus Aureus 90-95% and E. coli 65-70%. But these old antibiotics are only 12-18% sensitive for Pseudomonas species and 25 -55%. For Klebsiella species. A study on 126 patients in China in the year 2016 reported that gram-positive bacteria were susceptible to meropenem and imipenem, while sulbactam and ampicillin were nearly completely resistant.24 In another sample, 50% of the strains displayed an imipenem and meropenem sensitivity close to our sample.22
There is positive correlation of bacterial contamination between times elapsed since injury and debridement. Further multicentred and randomised study required to evaluate the nosocomial infection addressed in this study.
Conclusion
The study found Gustilo type III tibia fractures are predominant injury with highest infection rate. Surgical debridement is effective in reducing contamination from the open fracture wound, but the hospital-acquired infection is common in orthopaedic admitted patients where Gram-negative pathogens were dominant, and the antibiograms showed alarming pattern of drug resistance.
Acknowledgments
The authors express their gratitude to the institute and hospital where the research took place and to the all the participants who made it successful.
References
- Zalavras CG. Prevention of Infection in Open Fractures. Infectious disease clinics of North America. 2017;31:339- 52.
DOI: 10.1016/j.idc.2017.01.005 - Court-Brown CM, Bugler KE, Clement ND, Duckworth AD, McQueen MM. The epidemiology of open fractures in adults. A 15-year review. Injury. 2012;43:891-7.
DOI: 10.1016/j.injury.2011.12.007 - Neubauer T, Bayer GS, Wagner M. Open Fractures and Infection. Acta Chirurgiae Orthopaedicae Et Traumatologiae Èechosl. 2006;73:301-12.
PMID: 17140511 - Lee J. Efficacy of cultures in the management of open fractures. Clinical orthopaedics and related research. 1997;339:71-5.
DOI: 9186203 - Merritt K. Factors increasing the risk of infection in patients with open fractures. The Journal of trauma. 1988;28:823-7.
DOI: 3385826 - Al-Mulhim FA, Baragbah MA, Sadat-Ali M, Alomran AS, Azam MQ. Prevalence of surgical site infection in orthopedic surgery: a 5-year analysis. International surgery. 2014;99:264-68.
DOI: 10.9738/INTSURG-D-13-00251.1 - Malhotra AK, Goldberg S, Graham J, Malhotra NR, Willis MC, Mounasamy V, et al. Open extremity fractures: impact of delay in operative debridement and irrigation. The journal of trauma and acute care surgery. 2014;76:1201-7.
DOI: 10.1097/TA.0000000000000205 - Fernandes MDC, Peres LR, Neto ACDQ, Neto JQL, Turibio FM, Matsumoto MH. Open fractures and the incidence of infection in the surgical debridement 6 hours after trauma. Acta ortopedica brasileira. 2015;23:38-42.
DOI: 10.1590/1413-78522015230100932 - Zalavras CG, Marcus RE, Levin LS, Patzakis MJ. Management of open fractures and subsequent complications. The Journal of bone and joint surgery American volume. 2007;89:884-95.
DOI: 17432452 - Papakostidis C, Kanakaris NK, Pretel J, Faour O, Morell DJ, Giannoudis PV. Prevalence of complications of open tibial shaft fractures stratified as per the Gustilo-Anderson classification. Injury. 2011;42:1408-15.
DOI: 10.1016/j.injury.2011.10.015. - Weiss RJ, Montgomery SM, Ehlin A, Al Dabbagh Z, Stark A, Jansson KA. Decreasing incidence of tibial shaft fractures between 1998 and 2004: information based on 10,627 Swedish inpatients. Acta orthopaedica. 2008;79:526-33.
DOI: 10.1080/17453670710015535 - Spencer J, Smith A, Woods D. The effect of time delay on infection in open long-bone fractures: a 5-year prospective audit from a district general hospital. Annals of the Royal College of Surgeons of England. 2004;86:108-12.
DOI: 10.1308/003588404322827491 - Hannigan GD, Pulos N, Grice EA, Mehta S. Current Concepts and Ongoing Research in the Prevention and Treatment of Open Fracture Infections. Advances in wound care. 2015;4:59-74.
DOI: 10.1089/wound.2014.0531 - Clelland SJ, Chauhan P, Mandari FN. The epidemiology and management of tibia and fibula fractures at Kilimanjaro Christian Medical Centre (KCMC) in Northern Tanzania. The Pan African medical journal. 2016;25:51.
DOI: 10.11604/pamj.2016.25.51.10612. - Madadi F, Vahid Farahmandi M, Eajazi A, Daftari Besheli L, Madadi F, Nasri Lari M. Epidemiology of adult tibial shaft fractures: a 7-year study in a major referral orthopedic center in Iran. Medical science monitor : international medical journal of experimental and clinical research. 2010;16:CR217-21.
DOI: 20424548 - Ali A, Rahman M, Faruquee SR, Islam T, Rahim ZZ, Yusuf A. Treatment of open fracture of shaft of tibia-fibula Gustilo type III-B by SIGN interlocking nail and wound coverage by muscle flap within 72 hours of injury. International Journal of Research in Orthopaedics. 2017;3:898-03.
DOI: 10.18203/issn.2455-4510.IntJResOrthop20173931 - Guerra MTE, Gregio FM, Bernardi A, Castro CC. Infection rate in adult patients with open fractures treated at the emergency hospital and at the ULBRA university hospital in Canoas, Rio Grande do Sul, Brazil. Revista brasileira de ortopedia. 2017;52:544-8.
DOI: 10.1016/j.rboe.2017.08.012 - Yusof NM, Khalid KA, Zulkifly AH, Zakaria Z, Amin MA, Awang MS, et al. Factors associated with the outcome of open tibial fractures. The Malaysian journal of medical sciences : MJMS. 2013;20:47-53.
DOI: 24643115 - Johnson EN, Burns TC, Hayda RA, Hospenthal DR, Murray CK. Infectious complications of open type III tibial fractures among combat casualties. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America. 2007;45:409-15.
DOI: 10.1086/520029 - Matos MA, Catro-Filho RN, Silva BVPD. Risk factors associated with infection in tibial open fractures. Revista Facultad de Ciencias Medicas. 2013;70:14-8.
DOI: 23920097 - Elniel AR, Giannoudis PV. Open fractures of the lower extremity: Current management and clinical outcomes. EFORT open reviews. 2018;3:316-25.
DOI: 10.1302/2058-5241.3.170072 - Singh R, Sikka R, Maggu NK, Deep, Antrikshdeep, U. C, et al. Prevalence and antibiotic sensitivity pattern of bacteria isolated from nosocomial infections in orthopaedic patients. Journal of Orthopaedics 2010;7:e3.
DOI: 14710856 - Lingaraj R, Santoshi JA, Devi S, et al. Predebridement wound culture in open fractures does not predict postoperative wound infection: A pilot study. J Nat Sci Biol Med. 2015;6:S63-8.
DOI: 10.4103/0976-9668.166088 - Zhou C, Chen X, Wu L, Qu J. Distribution of drug-resistant bacteria and rational use of clinical antimicrobial agents. Experimental and therapeutic medicine. 2016;11:2229-32.
DOI: 10.3892/etm.2016.3239
Department of Orthopaedic Surgery, National Institute of Traumatology and Orthopaedic Rehabilitation, Dhaka, Bangladesh.
dssislam@yahoo.com
 0000-0001-8287-3347
0000-0001-8287-3347
Submission
04 April 2021
Accepted
30 June 2021
Published
01 August 2021
Apply citation style format of Bangladesh Medical Research Council
Issue
Vol 47 No 2 (2021)
Section
Research Articles
Ethical Clearance
IRB of NITOR, Dhaka, Bnagladesh.
Financial Support
Bangladesh Medical Research Council (BMRC), Dhaka.
Conflict of Interest
The authors declare no conflict of interest.